Wildfires have resulted in evacuations in some communities. Learn more.
Glossary
Cannabis – Cannabis is a broad term used to describe the various products derived from the leaves, flowers and resins of the Cannabis sativa and Cannabis indica plants, or hybrids of the two. These products exist in various forms and are used for different purposes (for example: medical, recreational, industrial).
Cannabis vs. marijuana – The federal government has adopted the term “cannabis” to describe cannabis products in general, as opposed to the commonly-used term “marijuana” (which only describes parts of the plant).
Cannabinoids – One of a class of chemical compounds that act on cannabinoid receptors in animals and humans, cannabinoids can be naturally extracted from cannabis plants. Over 104 different cannabinoids have been identified, with varied potencies depending on the plant or product. The most commonly-known cannabinoids are THC and CBD:
- THC (delta-9-tetrahydrocannabinol): has therapeutic effects and is the compound primarily responsible for the psychoactive effects of cannabis
- CBD (cannabidiol): has therapeutic but no psychoactive effects
Cannabis consumption – Cannabis can be used in many ways, some which may lead to second-hand smoke/vapour. Uses include:
- smoke (e.g., a joint, blunt, spliff, pipe, or bong)
- vaporize with a vaporizer (non-portable)
- vaporize with a vape pen or e-cigarette (portable)
- eat in food (e.g., brownies, cakes, cookies or candy)
- drink (e.g., tea, juice, cola, alcohol, other drinks)
- dab (e.g., applying to a hot surface with a metal tool)
- other (e.g., tinctures/drops under tongue, applied directly to skin in a lotion)
Impact on health
Recognizing the health risks of cannabis was a priority as we considered options for legalization.
While there is some understanding of the shorter-term risks of cannabis use (effects on memory, attention and psychomotor function) knowledge about long-term risks of cannabis use (permanent harm to mental functioning, risks of depression and anxiety disorders) is limited, mainly because cannabis use had been prohibited, so comprehensive studies have not been undertaken.
Health risks associated with cannabis use include:
- Risks to children and youth: Generally speaking, studies have consistently found that the earlier cannabis use begins and the more frequently and longer it is used, the greater the risk of potential developmental harms, some of which may be long-lasting or permanent.
- Risks associated with consumption: Certain factors are associated with an increased risk of harms, including frequent use and use of higher potency products. Driving while impaired by cannabis is associated with an increased risk of accidents and fatalities. Co-use with alcohol may pose an incremental risk for impaired driving and co-use with tobacco may increase smoking-related lung disease.
- Risks to vulnerable populations: Studies have found associations between frequent cannabis use and certain mental illnesses (e.g., schizophrenia and psychosis) and between frequent cannabis use during pregnancy and certain adverse cognitive and behavioural outcomes in children.
- Risks related to interactions with the illicit market: These include violence and the risks associated with unsafe products, illicit production and exposure to other, more harmful illicit substances.
Source: A Framework for the Legalization and Regulation of Cannabis in Canada.
Cannabis use in Alberta
In 2017, the University of Calgary published a study on cannabis consumption to inform Alberta’s response to the federal decision to legalize cannabis.
8.9% of Albertans (370,000) had used cannabis within the last 12 months, compared to a national average of 10.5%.
Since cannabis was not legal outside of the medical system, it’s likely the statistics were underestimated.
How Alberta compares: Canada and other countries
Chart 1: Cannabis use over 12-month period
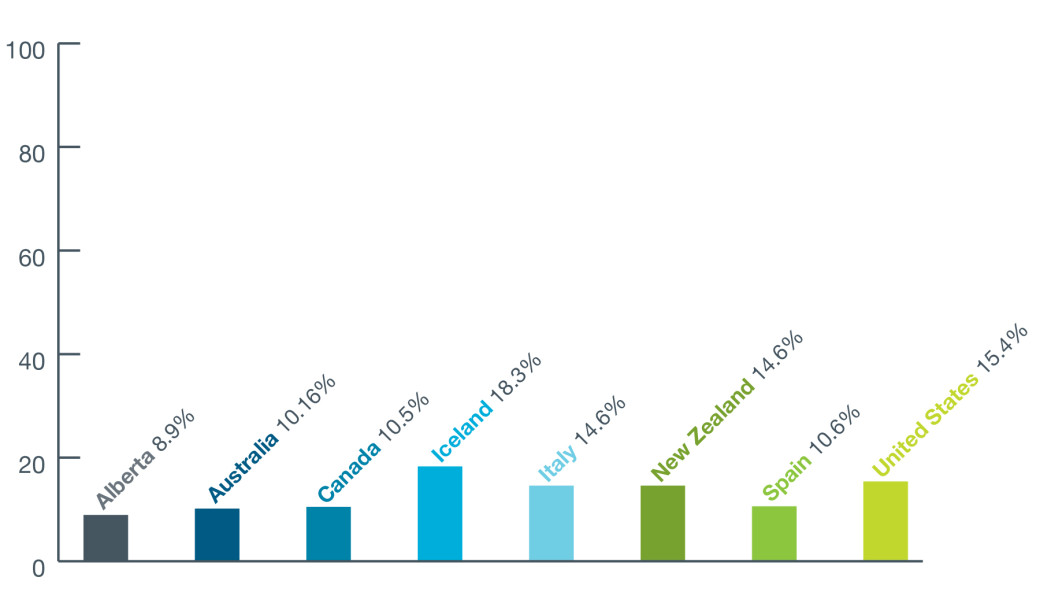
Alberta – 8.9%, Australia – 10.16%, Canada – 10.5%, Iceland – 18.3%, Italy – 14.6%, New Zealand – 14.6%, Spain – 10.6%, United States – 15.4%.
Source: University of Calgary, Cannabis Evidence Series, 2017
Source: University of Calgary, Cannabis Evidence Series, 2017
Other statistics
- In Alberta, cannabis use is lower than the national average, and the second-lowest provincial use rate, with 8.9% reporting use within the last 12 months.
- However, Alberta has amongst the highest lifetime use (37.3%), second only to Nova Scotia (42.4%). 33.7% of Canadians report lifetime use.
- In Canada, the prevalence of use within the last 12 months has decreased slightly since 2008 (11.7% in 2008 vs. 10.5% in 2013).
- Use declined across all provinces from 2008 to 2013, with the exception of BC.
Publications
Related
Previous
Cannabis legalization in Canada